
Pakistan is prone to devastating floods during the monsoon season. The flood affected population is at risk of both communicable and non-communicable diseases. The most common non-communicable diseases include injuries, animal and insect bites and mental health impacts, while infectious diseases specifically are associated with contaminated water/food or vector proliferation in the flood affected areas. This year, the population was still reeling from the effects of 2022 floods when Pakistan again experienced persistent rainfalls in April. This early summer rain resulted in another spell of floods that affected 18 districts (37%, 14/38) from Khyber Pakhtunkhwa and (12%, 4/36) from Baluchistan province. This posed a multitude of challenges such as population displacement and loss of precious lives due to injuries, exposure to communicable diseases, food insecurity, maternal and child health issues.

Image: Commuters drive through a flooded street after heavy monsoon rains in Larkana, Sindh province. Credit: Gulf Today
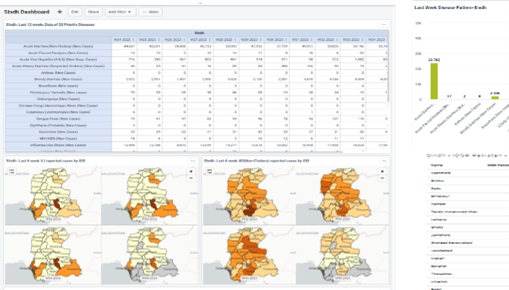
In response, the UKHSA International Health Regulations Strengthening Project (IHR-SP) team collaborated with the National Health Institute (NIH), affected provincial health departments and other stakeholders to rapidly establish a flood disease surveillance and response system. The system was built on existing Integrated Disease Surveillance and Response (IDSR) systems to enable presentation of accurate and timely data for evidence-based decisions. The National Command and Operation Centre (NCOC) subsequently approved the use of this system across the flood affected area in Pakistan. The new flood surveillance system enabled timely data collection (both manual and electronic through DHIS-2), established a flood dashboard, and regular situation reports to inform timely interventions for disease control and response.
Image: DHIS2 Dashboard Displaying 2024 Flood Data for Pakistan
The collaborative approach adopted in building this system between UKHSA, NIH and other partners was crucial in the development, deployment and dissemination of disease data. In addition, healthcare staff were trained in person and virtually on case definition and reporting, enabling standardisation of disease reporting. This training also helped the transition from routine weekly to emergency daily reporting which demonstrated the adaptability and flexibility of the IDSR system developed through IHR-SP. The DHIS-2 mobile application was also utilised to capture and share real time data. This real time data availability was instrumental for timely response.

The IDSR surveillance system was successfully utilised to respond to a public health emergency highlighting its robustness and agility. This proactive approach contributed significantly for timely identification of diseases and vulnerability of affected population including the geographic distribution. This significant new pivot of the IDSR in a public health emergency was appreciated nationally and internationally. It is anticipated that this experience will contribute to a sustainable data collection solution for emergency preparedness, particularly for emerging and rare diseases such as mpox.
Image: UKHSA IHR-SP Team Presenting Flood Data Collected via DHIS-2